Speech Sound Disorders-Articulation and Phonology
See the Speech Sound Disorders Evidence Map for summaries of the available research on this topic.
The scope of this page is idiopathic speech sound disorders (SSDs) with no known cause—historically called “articulation and phonological disorders”—in preschool and school-age children (ages 3–21 years). Idiopathic SSDs are typically identified in childhood. Information on this page may be relevant for idiopathic SSDs persisting into adulthood.
Information about speech sound problems related to motor/neurological disorders, structural abnormalities, and sensory/perceptual disorders (e.g., hearing loss) is not addressed on this page.
See ASHA’s Practice Portal pages on Childhood Apraxia of Speech and Cleft Lip and Palate for information about speech sound problems associated with these two disorders.
Speech sound disorders (SSDs) refer to any difficulty or a combination of difficulties with perception, motor production, or phonological representation of speech sounds and speech segments, including phonotactic rules governing permissible speech sound sequences in a language. Not all language(s) share the same speech sounds as mainstream American English. For children who use more than one language or dialect, the rules of one linguistic system may transfer and influence speech production in another. These influences do not indicate an SSD.
SSDs can be organic or idiopathic in nature. Organic SSDs result from motor/neurological disorders (e.g., childhood apraxia of speech, dysarthria), structural abnormalities (e.g., cleft lip/palate, other structural deficits or anomalies), and sensory/perceptual disorders (e.g., hearing loss). Idiopathic SSDs have no known cause. See the figure below.

Idiopathic SSDs
Idiopathic SSDs are disorders of the motor production of speech sounds and the linguistic aspects of speech production. These are referred to as articulation and phonological disorders, respectively. However, this page will refer to articulation and phonological disorders collectively as idiopathic SSDs.
Although the scope of this page is idiopathic SSDs, procedures and approaches described on this page may be appropriate for assessing and treating organic SSDs. See Speech Characteristics: Selected Populations [PDF] for a brief summary of selected populations and characteristic speech problems.
The incidence of speech sound disorders (SSDs) refers to the number of new cases identified in a specified period. The prevalence of SSDs refers to the number of children who are living with speech problems in a given time period.
The estimated prevalence rates of SSDs vary greatly due to the inconsistent classifications of the disorder and the variance of ages studied. There was also linguistic heterogeneity across the countries in which the studies mentioned below were conducted, which may lead to additional variability. Studies did not consistently report the linguistic profiles of the children or whether dialectal differences were considered for diagnosis. All these factors may lead to an overestimate of the number of children with a true SSD. The following data reflect the variability:
- Overall, 2.1%–23% of 4- to 6-year-old children were estimated to have SSDs (Eadie et al., 2015; Jessup et al., 2008; McKinnon et al., 2007).
- In 8-year-old children, 3.6% were estimated to have persistent SSDs (Wren et al., 2016).
- In young adults, 1%–2% exhibit residual or persistent speech errors (Flipsen, 2015).
- Reports estimated that SSDs are more prevalent in boys than in girls, with a ratio of about 2:1 in grade school children (McKinnon et al., 2007). There were no indications whether the data collected were based on sex assigned at birth and/or gender identity.
- Lower socioeconomic status was associated with SSDs in some studies, but not others (Eadie et al., 2015; McKinnon et al., 2007).
- Reports estimated that 40% of children with SSDs had concomitant language impairment (Eadie et al., 2015).
- Approximately 8% of children with SSDs also stutter (Unicomb et al., 2020).
- Poor speech sound production skills in kindergarten children have been associated with lower literacy outcomes, especially in children with concomitant language or phonological awareness difficulties (Hayiou-Thomas et al., 2017; Overby et al., 2012; Peterson et al., 2009). Approximately 25% of children receiving school-based speech services may also qualify for reading-related services (Tambyraja et al., 2020).
Signs and symptoms of idiopathic speech sound disorders include the following:
- Omissions/deletions—Certain sounds are omitted or deleted (e.g., /kʌ/ for “cup” and /pun/ for “spoon”).
- Substitutions—One or more sounds are substituted, which may result in loss of phonemic contrast (e.g., /θɪŋ/ for “sing” and /wæbɪt/ for “rabbit”).
- Additions—One or more extra sounds are added or inserted into a word (e.g., /bəlæk/ for “black”).
- Distortions—Sounds are altered or changed (e.g., a lateral /s/).
- Syllable-level errors—Weak syllables are deleted (e.g., /tɛfoʊn/ for “telephone”).
- Inconsistent whole-word productions—The same word is produced differently across repetitions (e.g., “strawberry” as /sɔbi/, /ʃɔbɛwi/, or /tɔbɹi/) in the absence of motor speech difficulties.
Signs and symptoms may occur as independent articulation errors and/or phonological rule-based error patterns (see ASHA’s resource on selected phonological patterns for examples). In addition to these common rule-based error patterns, unique error patterns can also occur. For example, a child might substitute many sounds with a favorite or default sound, resulting in several homonyms (e.g., “shore,” “sore,” “chore,” and “tore” might all be pronounced as /dɔɹ/; Grunwell, 1987; Williams, 2003a).
Consideration of Communication Profiles
We all speak with an accent and use one or more dialects. Analysis of speech sounds begins with consideration of linguistic systems used. The clinician considers speech sounds, patterns, and rules that are part of the linguistic system(s) of the child. Heritage language(s) can influence the pronunciation of speech sounds and the acquisition of phonotactic rules in the additional language(s) used.
Accents are systematic variations in speech production marked by differences in phonological and/or prosodic features, including rate and fluency, that are perceived as different from any native, mainstream, regional, or dialectal form of speech (Celce-Murcia et al., 1996; Valles, 2015). These linguistic variations may affect intelligibility for unfamiliar listeners. However, someone can have a noticeable accent and still be intelligible. See ASHA’s Practice Portal pages on Multilingual Service Delivery in Audiology and Speech-Language Pathology and Cultural Responsiveness.
Dialects are rule-governed language systems that reflect the regional and social background of its speakers. These rules cross all linguistic parameters, including phonology, morphology, syntax, semantics, and pragmatics. Rules across these linguistic parameters may influence speech sound production. For example, a morphological rule of a dialect to mark a plural by number (e.g., “I see six dog”) rather than using a final /s/ could be misattributed as a phonological error pattern instead of a dialectical difference. Familiarity with the rules of a dialect is critical in determining expectations for speech sounds within the linguistic profile of a person.
See ASHA’s Practice Portal pages on Accent Modification, Multilingual Service Delivery in Audiology and Speech-Language Pathology, and Cultural Responsiveness.
The cause of idiopathic speech sound disorders (SSDs) is not known; however, some risk factors have been investigated.
Frequently reported risk factors include the following:
- Biological sex—The incidence of SSDs is higher in males than in females assigned at birth (e.g., Everhart, 1960; Morley, 1952; Shriberg et al., 1999).
- Pre- and perinatal problems—Factors such as maternal stress or infections during pregnancy, complications during delivery, preterm delivery, and low birthweight were found to be associated with delay in speech sound acquisition and with SSDs (e.g., Brown et al., 1986; Fox et al., 2002).
- Family history—Children who have family members (parents or siblings) with speech and/or language difficulties were more likely to have a speech disorder (e.g., Campbell et al., 2003; Felsenfeld et al., 1995; Fox et al., 2002; Shriberg & Kwiatkowski, 1994).
- Persistent otitis media with effusion—Persistent otitis media with effusion (often associated with hearing loss) has been associated with impaired speech development (Fox et al., 2002; Silva et al., 1986; Teele et al., 1990).
Protective factors, social risk factors, and social needs can also influence outcomes. Some of these factors include access to early intervention and resources, language-rich environments, access to health care, and parental education and engagement. Visit ASHA’s resource on social determinants of health for more information.
Speech-language pathologists (SLPs) play a central role in the screening, assessment, diagnosis, and treatment of children with speech sound disorders (SSDs). The professional roles and activities in speech-language pathology include clinical/educational services (diagnosis, assessment, planning, and treatment); prevention and advocacy; and education, administration, and research. See ASHA’s Scope of Practice in Speech-Language Pathology (ASHA, 2016).
Appropriate roles for SLPs are as follows.
Education
- Provide information on prevention to people known to be at risk for SSDs.
- Educate other professionals on the needs of people with SSDs and the role of SLPs in diagnosing and managing SSDs.
- Remain informed of research in the area of SSDs, help advance the knowledge base related to the nature and treatment of these disorders, and use evidence-based research to guide intervention.
Screening and Assessment
- Screen individuals who present with speech sound difficulties and determine the need for further assessment and/or referral for other services.
- Recognize that students with SSDs have heightened risks for later language and literacy problems.
- Conduct a culturally and linguistically relevant comprehensive assessment of speech, language, and communication.
- Consider the rules of a spoken accent or dialect, typical dual-language acquisition from birth, and sequential second-language acquisition to be able to identify a potential disorder within linguistic profiles.
- Diagnose the presence or absence of an SSD within linguistic profiles.
- Refer to and collaborate with other professionals to rule out other conditions, determine etiology, and facilitate access to comprehensive services.
Intervention and Support
- Make person-centered and culturally responsive decisions about the management of SSDs.
- Make decisions about eligibility for services based on the presence of an SSD.
- Develop treatment plans, provide intervention and support services, document progress, and determine appropriate service delivery approaches and dismissal criteria.
- Counsel people with SSDs and their families/caregivers regarding communication-related issues and provide education aimed at preventing further complications related to SSDs.
- Serve as an integral member of an interdisciplinary team working with individuals with SSDs and their families/caregivers (see ASHA’s resource on interprofessional education/interprofessional practice [IPE/IPP]).
- Consult and collaborate with professionals, family members, caregivers, and others to facilitate program development and to provide supervision, evaluation, and/or expert testimony (see ASHA’s resource on focusing care on individuals and their care partners).
- Advocate for individuals with SSDs and their families at the local, state, and national levels.
As indicated in the ASHA Code of Ethics (ASHA, 2023), SLPs who serve this population should be specifically educated and appropriately trained to do so.
See the Assessment section of the Speech Sound Disorders Evidence Map for pertinent scientific evidence, expert opinion, and client/caregiver perspective.
Screening
Screening is conducted whenever a speech sound disorder (SSD) is suspected or part of a comprehensive speech and language evaluation for a child with communication concerns. The language of the screening is in the language normally used by the child in the home or learning environment (Individuals with Disabilities Education Improvement Act of 2004 [IDEA]). The purpose of the screening is to identify if a child requires speech-language assessment and/or referral for other professional services.
Screening typically includes
- screening of individual speech sounds in single words and connected speech (using formal and/or informal screening measures),
- screening of oral motor functioning (e.g., range of motion of oral musculature),
- an orofacial examination to assess facial symmetry and identify possible structural bases for SSDs (e.g., submucous cleft palate, malocclusion, ankyloglossia), and
- an informal assessment of language comprehension and production.
See ASHA’s resource on assessment tools, techniques, and data sources.
Screening may result in
- determination that speech is appropriate for a child’s age and/or linguistic community;
- recommendation to monitor speech and rescreen;
- referral for multi-tiered systems of support (MTSS), such as response to intervention (RTI);
- referral for a comprehensive speech sound assessment;
- recommendation for a comprehensive language assessment, if language delay or a language disorder is suspected;
- referral to an audiologist for a hearing evaluation, if hearing loss is suspected; and
- referral for medical or other professional services, as appropriate.
Comprehensive Assessment
The acquisition of speech sounds is a developmental process. Children often demonstrate “typical” errors and phonological patterns during this learning period. Developmental patterns vary across linguistic systems. Speech-language pathologists (SLPs) analyze whether those patterns are typical within the child’s linguistic community or the patterns are unexpected and not age appropriate within the linguistic community.
Assessment includes a variety of measures and activities, including administration of standardized and nonstandardized measures as well as formal and informal assessment tools. See ASHA’s resource on assessment tools, techniques, and data sources.
SLPs are familiar with nondiscriminatory testing and dynamic assessment procedures, such as identifying the potential sources of test bias, administering and scoring standardized tests using alternative methods, and analyzing test results considering existing information regarding dialect use (see, e.g., McLeod et al., 2017). For example, assessment results can be biased because the photos and/or images used to elicit sounds may not be culturally relevant to the student. Clinicians probe unanticipated response(s) to determine if an alternative prompt may be more relevant to elicit a response. SLPs who speak a language different from the client’s or the student’s language might work with an interpreter for assessment procedures. See ASHA’s Practice Portal page on Collaborating with Interpreters, Transliterators, and Translators. SLPs are knowledgeable of shared versus unshared sounds in the languages being evaluated.
Standard scores cannot be reported for assessments that are not normed on a group that is representative of the individual being assessed. Documentation should include reporting, which provides a rich description of the child’s communication profile with consideration of the language(s) and dialect(s) used. The presence of an SSD may not be determined by comparison to mainstream American English (MAE) but, rather, from looking at the rules and influences of speech sound production of the language(s), accent(s), and/or dialect(s) used by the student.
The variables to consider are as follows:
- phonemic and allophonic variations of the language(s) and/or dialect(s) used in the community
- the rules and linguistic features of language(s) and/or dialect(s) and how they may influence speech sound production
- the influence of SSDs, accents, dialects, and patterns of transfer from one language to another
See ASHA’s resource on phonemic inventories and cultural and linguistic information across languages.
Consistent with the World Health Organization’s (WHO’s) International Classification of Functioning, Disability and Health (ICF) framework (ASHA, 2016; WHO, 2001), a comprehensive assessment is conducted to identify and describe impairments, functioning, disability, and contextual factors.
See ASHA’s Person-Centered Focus on Function: Speech Sound Disorder [PDF] for an example of assessment data consistent with the ICF framework.
Assessment may result in one or more the following:
- determination that their speech is appropriate for their age and/or linguistic community
- diagnosis of SSD
- description of the characteristics, subtype, and severity of the disorder
- recommendations for intervention targets
- identification of factors that might contribute to the SSD
- recommendation for additional spoken and/or written language assessment
- recommendation to monitor reading and writing progress in students with identified SSDs by SLPs and other professionals in the school setting
- referral for MTSS, such as RTI, to support speech and language development
- referral to other professionals, as needed
MTSS
Students screened for SSDs may not qualify for speech-language services under IDEA but may benefit from additional support in the general education setting through MTSS (Bruce et al., 2018; Flipsen & Sacks, 2022; Swaminathan & Farquharson, 2018). MTSS are a data-driven framework to support the academic, behavioral, emotional, and social success of all students in the general and special education settings (Center on Multi-Tiered System of Supports, n.d.). Essential components of MTSS include universal screening, progress monitoring, data-based decision making, and a multilevel prevention system (Center on Multi-Tiered System of Supports, n.d.). MTSS can help SLPs with service delivery and interprofessional collaboration (Sylvan, 2023).
RTI is an example of a three-tiered MTSS framework [PDF]. SLPs can work within the RTI process to identify children with SSDs and to provide instruction to struggling students.
RTI cannot be used to delay or deny an evaluation to determine if a student is eligible to receive special education and related services under the IDEA (Office of Special Education and Rehabilitative Services, 2011).
See ASHA’s resource on RTI for more information about how SLPs can be part of the RTI process.
Case History
The case history typically includes gathering information about
- the family’s concerns about the child’s speech, language, and literacy skills;
- the history of middle ear infections;
- the family history of speech and language difficulties (including reading and writing);
- the language(s) and dialect(s) used in the home;
- the primary language(s) and dialect(s) spoken by the child;
- the family’s and other communication partners’ perceptions of intelligibility (see the Resources section for related tools); and
- the teacher’s report of the child’s intelligibility, the child’s participation in the school setting, and how the child’s speech compares with that of peers in the classroom.
See ASHA’s Practice Portal page on Cultural Responsiveness for guidance on taking a case history with all clients.
Oral Mechanism Examination
The oral mechanism examination evaluates the structure and function of the physical speech mechanism to assess whether the system is adequate for speech production. This examination typically includes assessment of
- dental occlusion and specific tooth deviations;
- the structure of hard and soft palate (clefts, fistulas, bifid uvula); and
- the function (range of motion) of the lips, jaw, tongue, and velum.
Hearing Screening
A hearing screening is conducted during the comprehensive speech sound assessment, if one was not completed during the screening.
Hearing screening typically includes
- an otoscopic inspection of the ear canal and tympanic membrane,
- pure-tone audiometry, and
- immittance testing to assess middle ear function.
Speech Sound Assessment
The speech sound assessment uses both standardized assessment instruments, as appropriate, and other sampling procedures to evaluate production in single words and connected speech. Criterion-referenced assessment procedures can be also used to add to an accurate profile of the child’s speech skills, especially for children who use more than one language (Fabiano-Smith, 2019).
Single-word testing provides identifiable units of production and allows most consonants in the language to be elicited in various phonetic contexts; however, it may or may not reflect the same sound production as connected speech.
Connected speech sampling provides information about the production of sounds in connected speech. Activities to elicit a connected speech sample may include storytelling or retelling, describing pictures, and normal conversations about a topic of interest.
Assessment of speech includes an evaluation of the following:
- Accurate productions
- sounds in various word positions (e.g., initial-word, within-word, and final-word positions) and in different phonetic contexts
- sound combinations (e.g., vowel combinations, consonant clusters)
- syllable shapes (e.g., from simple consonant–vowel to complex consonant–consonant–vowel–consonant–consonant)
- Speech sound errors
- error types (e.g., deletions, omissions, substitutions, distortions, additions)
- error distribution (e.g., position of the sound in a word)
- error patterns (i.e., phonological patterns)—systematic sound changes or simplifications that affect a class of sounds (e.g., fricatives), sound combinations (e.g., consonant clusters), or syllable structures (e.g., complex syllables or multisyllabic words)
- consistency of errors (e.g., inconsistent vs. consistent errors, whole-word variation of errors)
See Crowe and McLeod’s (2020) Consonant Age of Acquisition [PDF], ages of acquisition of consonants in African American English (Pearson et al., 2009; Velleman & Pearson, 2010), and ASHA’s resource on selected phonological patterns.
Severity Assessment
Severity is a qualitative judgment made by the clinician. It indicates the impact of the SSD on functional communication. It is typically defined along a continuum from mild to severe or profound. There is no clear consensus regarding the best way to determine the severity of an SSD—rating scales and quantitative measures have been used.
A numerical scale or continuum of disability is often used because it is time efficient. Prezas and Hodson (2010) use the following continuum of severity:
- mild—rare omissions and few substitutions
- profound—extensive omissions and many substitutions; extremely limited phonemic and phonotactic repertoires
Distortions and assimilations occur in varying degrees at all levels of the continuum above.
A quantitative approach (Shriberg & Kwiatkowski, 1982a, 1982b) uses the percentage of consonants correct to determine severity on a continuum from mild to severe. To determine the percentage of consonants correct, collect and phonetically transcribe a speech sample. Then, count the total number of consonants in the sample and the total number of correct consonants (Shriberg et al., 1997).
Intelligibility Assessment
Intelligibility is a perceptual judgment based on how much of the child’s spontaneous speech the listener understands. Intelligibility can vary along a continuum ranging from intelligible (message is completely understood) to unintelligible (message is not understood; Bernthal et al., 2022). SLPs frequently use intelligibility to judge the severity of the child’s speech problem and to determine the need for intervention (McLeod et al., 2012; Mullen & Schooling, 2010).
Intelligibility can vary depending on several of the following factors:
- the number, type, and frequency of speech sound errors (when present)
- the speaker’s rate, inflection, stress patterns, pauses, voice quality, loudness, and fluency
- linguistic factors (e.g., word choice and grammar)
- the complexity of the utterance (e.g., single words vs. conversational or connected speech)
- the listener’s familiarity with the speaker’s speech pattern
- communication environment (e.g., familiar vs. unfamiliar communication partners, one-on-one vs. group conversations)
- communication cues for the listener (e.g., nonverbal cues from the speaker, including gestures and facial expressions)
- signal-to-noise ratio (i.e., amount of background noise)
Rating scales and other estimates that are based on perceptual judgments are commonly used to assess intelligibility. Rating scales sometimes use numerical ratings such as 1 for totally intelligible and 10 for unintelligible. Some rating scales use descriptors such as not at all, seldom, sometimes, most of the time, or always to indicate how well speech is understood (Ertmer, 2010). A parent-rated scale can provide a picture of the child’s intelligibility in different contexts and listeners (McLeod et al., 2012).
Several quantitative measures have been also proposed, including calculating the percentage of words understood in conversational speech (e.g., Flipsen, 2006; Shriberg & Kwiatkowski, 1980). See also Kent et al. (1994) for a comprehensive review of procedures for assessing intelligibility.
Intelligibility can vary depending on context and the familiarity of listeners. Coplan and Gleason (1988) developed a standardized intelligibility screener using parent estimates of how intelligible their child sounded to others. Based on the study’s data, expected intelligibility cutoff values for English-speaking children without SSDs were as follows:
- 22 months—50%
- 37 months—75%
- 47 months—100%
Hustad et al. (2021) investigated intelligibility in children without SSDs—from 2;6 (years;months) to 9;11 of age. All the children were monolingual American English speakers, and most of the participants were White. With unfamiliar listeners, the average intelligibility thresholds of context-free single words for children without SSDs were as follows:
- 31 months—50%
- 49 months—75%
- 83 months—90%
See the Resources section for more resources related to assessing intelligibility and life participation in monolingual children across several languages and dialects of English.
Stimulability Testing
Stimulability is the child’s ability to accurately imitate a model of the target speech sound that the child currently misarticulates. There are few standardized procedures for testing stimulability (Glaspey & Stoel-Gammon, 2007; Powell & Miccio, 1996), although some test batteries include stimulability subtests.
Stimulability testing helps determine
- how well the child imitates the sound in one or more contexts (e.g., isolation, syllable, word, phrase),
- whether the sound is likely to be acquired without intervention, and
- which targets are appropriate for therapy (Tyler & Tolbert, 2002).
Speech Perception Testing
Speech perception is the ability to perceive acoustic differences between speech sounds. Speech perception difficulties are common in children with SSDs (Cabbage, 2015; Hearnshaw et al., 2019). In children with SSDs, speech perception is the child’s ability to perceive the difference between the target production of a sound and their own error production or to perceive the contrast between two phonetically similar sounds (e.g., ɹ/w, s/ʃ, f/θ).
The SLP also needs to know how the child’s linguistic community—the influences of the child’s receptive and expressive language—pronounces a word. For example, the SLP asks the child whether /goʊld/ is pronounced correctly or incorrectly. In speech perception tasks, a child might indicate /goʊld/ as incorrect because their linguistic community pronounces the first consonant of the final consonant cluster (i.e., “gold” as /goʊl/; Shollenbarger et al., 2017).
Speech perception abilities can be tested using the following methods:
- Auditory discrimination—Syllable pairs containing a single phoneme contrast are presented, and the child is instructed to say “same” if the paired items sound the same and “different” if they sound different.
- Picture identification—The child is shown two to four pictures representing words with minimal phonetic differences. The clinician says one of these words, and the child is asked to point to the correct picture.
- Pronunciation accuracy/inaccuracy
- Speech production–perception task—Using sounds that the child is suspected of having difficulty perceiving, picture targets containing these sounds are used as visual cues. The child is asked to judge whether the speaker says the item correctly (e.g., the picture of a ship is shown, and the speaker says “/ʃɪp/” or “/sɪp/”; Locke, 1980).
- Mispronunciation detection task—Using picture stimuli and recorded or live stimulus names (either correct or with a single phoneme error), the child is asked to detect mispronunciations by pointing to a green tick for “correct” or a red cross for “incorrect” (McNeill & Hesketh, 2010).
- Lexical decision/judgment task—Using target pictures and single-word recordings, this task assesses the child’s ability to identify words that are pronounced correctly or incorrectly. A picture of the target word (e.g., “lake”) is shown, along with a recorded word—either /leɪk/ or a word with a contrasting phoneme (e.g., /weɪk/). The child points to the picture of the target word if it was pronounced correctly or to an “X” if it was pronounced incorrectly (Rvachew et al., 2004).
Considerations for Assessing Young Children and/or Children Who Are Reluctant or Have Less Intelligible Speech
Some children might not be able to follow directions for standardized tests, might have limited expressive vocabulary, or might produce words that are unintelligible. Other children, regardless of age, may produce less intelligible speech or be reluctant to speak in an assessment setting.
Examples of strategies for collecting an adequate speech sample with these populations are as follows:
- having play activities during the assessment session
- naming, or telling a story about, pictures or toys for a communication sample
- involving families/caregivers in the session to encourage talking
- asking families/caregivers to supplement data from the assessment session by recording the child’s speech at home during spontaneous conversations
- asking parents/caregivers to keep a log of the child’s intended words and how these words are pronounced
Sometimes, the SSD is so severe that the child’s intended message cannot be understood. However, even when a child’s speech is unintelligible, it is usually possible to obtain information about their speech sound production.
For example:
- A single-word articulation test provides opportunities for the production of identifiable units of sound, and these productions can be usually transcribed.
- It may be possible to understand and transcribe a spontaneous speech sample by (a) using a structured situation to provide context when obtaining the sample and (b) annotating the recorded sample by repeating the child’s utterances, when possible, to facilitate later transcription.
Differential Diagnosis of Idiopathic SSDs and Childhood Apraxia of Speech
The SLP may need to distinguish a subtype of idiopathic SSDs (e.g., consistent phonological error patterns, inconsistent phonological error patterns) and childhood apraxia of speech (CAS). Consistent phonological error patterns are characterized by predictable errors and weak phonological processing (Rvachew & Matthews, 2024). Inconsistent phonological error patterns are characterized by weak phonological planning and inconsistent whole-word errors (Rvachew & Matthews, 2024). For example, the same person might pronounce “strawberry” as /sɔbi/, /ʃɔbɛwi/, or /tɔbɹi/ during different repetitions. CAS is characterized by weak motor planning and lexical stress errors (Murray et al., 2021; Rvachew & Matthews, 2024).
Differential diagnosis of a severe SSD from CAS can be challenging (Murray et al., 2021). There is no single measure that can provide a sufficient true negative (sensitivity) or true positive (specificity). Therefore, the clinician uses combinations of measures and markers. For example, inconsistency, segmental accuracy, and prosody measures have high specificity but low sensitivity (Murray et al., 2021; Strand et al., 2013).
See Speech Characteristics: Selected Populations [PDF] for a brief summary of the characteristics of CAS. See also ASHA’s Practice Portal page on Childhood Apraxia of Speech.
Considerations for Multilingual and Multidialectal Populations
Assessment of a multilingual individual requires an analysis of linguistic systems. Determination of the presence of an SSD is made by examining the rules and patterns within the linguistic systems used and not by comparison to MAE. Every language consists of multiple dialects. Some people only use a dialect of MAE and do not use MAE at all. Upon gathering data, clinicians may need to examine responses to determine if they reflect a dialectal variation within that language. There are additional considerations for the clinician to consider.
Prior to evaluation, the clinician gathers linguistically relevant information, including
- the phonemic inventory, phonological structure, and syllable structure of the language(s) and/or dialect(s) used;
- the morphological and syntactic rules of the language(s) and/or dialect(s); and
- additional information about the language(s) and dialect(s) used, by collaborating with a linguistic broker, as needed.
Cross-linguistic studies reveal that while there may be some patterns in speech sound development, milestones for phonemic development vary. These variations continue as children develop multiple languages and/or dialects. Clinicians consider what is linguistically relevant for the child in establishing expectations for speech sound development. Multilingual children might use translanguaging to communicate. In translanguaging, the speaker may fluctuate between features of and across languages using the linguistic features available to them in their communication profile. Translanguaging is not a sign of a communication disorder.
Pertinent data to consider during evaluation are as follows:
- detailed linguistic history for multilingual children
- age each language was introduced
- language(s) that the child uses to communicate in the home, with caregivers, and with peers
- how often the child uses each language
- modification of assessments
- allow for response(s) in all languages and/or dialects used
- allow for translanguaging in connected speech samples
Clinicians identify and assess patterns that reflect cross-linguistic effects. A disorder exists if the speech sound features used by the child do not reflect the patterns of the languages and/or dialects the child is familiar with or uses.
Analysis of data and subsequent documentation centers around the child’s communication profile. In multilingual and/or multidialectal children, comparison of production to MAE language norms and syntactic rules does not provide clarity in determining the potential presence of an SSD.
See ASHA’s resource on phonemic inventories and cultural and linguistic information across languages and ASHA’s Practice Portal page on Multilingual Service Delivery in Audiology and Speech-Language Pathology. See the Resources section for information related to assessing intelligibility and life participation in monolingual children who speak English and those who speak languages other than English.
Phonological Processing Assessment
Phonological processing is the use of sounds of one’s language (i.e., phonemes) to process spoken and written language (Wagner & Torgesen, 1987). The broad category of phonological processing includes phonological awareness, phonological working memory, and phonological retrieval.
All three components of phonological processing are important for speech production and for the development of spoken and written language skills. Phonological processing difficulties are predictive of difficulties in reading and reading-related skills (Tambyraja et al., 2020; Walquist-Sørli et al., 2025). Therefore, it is important to assess phonological processing skills and to monitor the spoken and written language development of children with phonological processing difficulties.
- Phonological awareness is the awareness of the sound structure of a language and the ability to consciously analyze and manipulate this structure via a range of tasks, such as speech sound segmentation and blending at the word, onset–rime, syllable, and phonemic levels.
- Phonological working memory involves storing phoneme information in a temporary short-term memory store (Wagner & Torgesen, 1987). This phoneme information is then readily available for manipulation during phonological awareness tasks. Nonword repetition (e.g., repeat “/pæɡ/”) is one example of a phonological working memory task.
- Phonological retrieval is the ability to retrieve phonological information from long-term memory. It is typically assessed using rapid naming tasks (e.g., rapid naming of objects, colors, letters, or numbers). This ability to retrieve the phonological information of one’s language is integral to phonological awareness.
Phonological processing tasks often rely on spoken responses. Therefore, some phonological processing tasks may not accurately reflect the phonological processing skills of children with SSDs because of their speech errors (Roepke, 2024). SLPs consider the following methods to ensure that speech production errors do not impact spoken measures (Roepke, 2024):
- Receptive tasks, such as “Do /bæt/ and /mæt/ start with same sound?” or pointing to the pictures that start with the target sound.
- Only including sounds that the child can produce accurately.
- Excluding sounds that the child produces incorrectly when calculating the score.
- Knowing how aware a child is of their speech production errors. The child may take extra time to produce target sounds.
Linguistic variations in pronunciation may influence responses to prompts. Clinicians familiarize themselves with the child’s linguistic system to understand rules and sound production that could influence phonological processing tasks (Shollenbarger et al., 2017). See Roepke (2024) for more information on assessment approaches for phonological processing skills in children with SSDs.
Language Assessments
Language testing is included in a comprehensive speech sound assessment because of the high incidence of co-occurring language problems in children with SSDs (Shriberg & Austin, 1998).
Spoken Language Assessment (Listening and Speaking)
A full spoken language assessment battery is performed if indicated by screening results. See ASHA’s Practice Portal page on Spoken Language Disorders for more details.
It may be difficult for children with specific speech errors (e.g., final-consonant deletion) to complete language assessments. It may also be difficult for SLPs to understand highly unintelligible children with SSDs on a language sample. SLPs may choose to use receptive language assessments or sentence imitation tasks (see Seeff-Gabriel et al., 2010) when working with children with SSDs.
Written Language Assessment (Reading and Writing)
For children without SSDs, speech production and phonological awareness develop in a mutually supportive way (Carroll et al., 2003; National Institute for Literacy, 2009). As children playfully engage in sound play, they eventually learn to segment words into separate sounds and to “map” sounds onto printed letters.
Difficulties with the speech processing system—such as listening and discriminating or remembering speech sounds—can lead to speech production and literacy-related difficulties. Difficulties in these areas can have a negative impact on the development of reading and writing skills (Anthony et al., 2011; Catts et al., 2017; Leitão & Fletcher, 2004; Lewis et al., 2011; Walquist-Sørli et al., 2025). Even children with mild SSDs can have an increased risk of literacy-related difficulties, such as phonological awareness and spelling (Farquharson, 2019).
See ASHA’s Practice Portal page on Written Language Disorders for more details.
See the Treatment section of the Speech Sound Disorders Evidence Map for pertinent scientific evidence, expert opinion, and client/caregiver perspective.
It is often difficult to clearly differentiate between articulation and phonological errors or to differentially diagnose these as two separate disorders. A single child might show both articulation and phonological error types. Those specific errors might need different treatment approaches.
Treatment of speech sound disorders (SSDs) typically involves the following sequence of steps:
- establishment—eliciting target sounds and stabilizing production on a voluntary level
- generalization—facilitating carryover of sound productions at increasingly challenging levels (e.g., syllables, words, phrases/sentences, conversational speaking)
- maintenance—stabilizing target sound production and making it more automatic; encouraging self-monitoring of speech and self-correction of errors
Target Selection
Approaches for selecting initial therapy targets for children with SSDs include the following:
- Client-specific—Target sounds are selected based on factors such as relevance to the child and their family (e.g., sound is in the child’s name), stimulability, and/or visibility when produced (e.g., /f/ vs. /k/).
- Degree of deviance and impact on intelligibility—Target sounds are selected based on errors (e.g., omission, initial-consonant deletion) that most affect intelligibility.
- Developmental—Target sounds are selected based on the order of acquisition in typically developing children.
- Theoretically motivated, including the following:
- Complexity—focuses on more complex, linguistically marked phonological elements not in the child’s phonological system to encourage cascading, generalized learning of sounds (Gierut, 2007; Storkel, 2018). These include hierarchies of complexity (e.g., clusters, fricatives, and affricates are more complex than other sound classes) and stimulability (i.e., sounds with the lowest levels of stimulability are most complex). See Baker and Williams (2010) and Peña-Brooks and Hegde (2023) for detailed descriptions of the complexity approach.
- Dynamic systems—focuses on teaching and stabilizing simple target phonemes that do not introduce new feature contrasts in the child’s phonological system to assist in the acquisition of target sounds and more complex targets and features (Rvachew & Bernhardt, 2010).
- Systemic—focuses on the function of the sound in the child’s phonological organization to achieve maximum phonological reorganization with the least amount of intervention. Target selection is based on a distance metric. Targets can be maximally distinct from each other and the child’s error in terms of place, voice, and manner (Williams, 2003b). For example, the SLP might target voiced versus voiceless fricatives and affricates if the child uses /h/ for multiple phonemes (Storkel, 2022). See Roth and Worthington’s (2018) Place, Manner, and Voicing Chart for English Consonants [PDF].
See ASHA’s Person-Centered Focus on Function: Speech Sound Disorder [PDF] for an example of goal setting consistent with the ICF framework.
Treatment Strategies
In addition to selecting appropriate targets for intervention, speech-language pathologists (SLPs) select treatment strategies based on the number of intervention goals addressed in each session and the way these goals are implemented. A particular strategy may not be appropriate for all children, and strategies may change throughout the course of intervention as the child’s needs change.
“Target attack” strategies include the following:
- Vertical—intense practice on one or two targets until the child reaches a specific criterion level (usually conversational level) before proceeding to the next target or targets (see, e.g., Fey, 1986).
- Horizontal—less intense practice on a few targets. Multiple targets are addressed individually or interactively in the same session, thus providing exposure to more aspects of the sound system (see, e.g., Fey, 1986).
- Cyclical—incorporating elements of both horizontal and vertical structures. The child is provided with practice on a given target or targets for some predetermined period of time before moving on to another target or targets for a predetermined period of time. Practice then cycles through all targets again (see, e.g., Hodson, 2010).
Treatment Options
The following are brief descriptions of both general and specific treatments for children with SSDs. These approaches can be used to treat speech sound problems in a variety of populations. See Speech Characteristics: Selected Populations [PDF] for a brief summary of selected populations and characteristic speech problems.
Treatment selection depends on several factors, including the child’s age, the type of speech sound errors, the severity of the disorder, and the degree to which the disorder affects overall intelligibility (Williams et al., 2010). This list is not exhaustive, and inclusion does not imply endorsement from ASHA. For multilingual children, SLPs consider the communication strengths and needs in all languages and dialects.
For additional information and considerations, please see ASHA’s Practice Portal page on Multilingual Service Delivery in Audiology and Speech-Language Pathology.
Contextual Utilization Approaches
Contextual utilization approaches recognize that speech sounds are produced in syllable-based contexts in connected speech and that some (phonemic/phonetic) contexts can facilitate correct production of a particular sound.
Contextual utilization approaches may be helpful for children who use a sound inconsistently and need a method to facilitate consistent production of that sound in other contexts. Instruction for a particular sound is initiated in the syllable context(s) where the sound can be produced correctly (McDonald, 1974). The syllable is used as the building block for practice at more complex levels.
For example, the production of a /t/ may be facilitated in the context of a high front vowel, as in “tea” (Bernthal et al., 2022). Facilitative contexts or “likely best bets” for production can be identified for voiced, velar, alveolar, and nasal consonants. For example, a “best bet” for nasal consonants is before a low vowel, as in “mad” (Bleile, 2002).
Core Vocabulary Approach
A core vocabulary approach focuses on whole-word production and is used for children with inconsistent whole-word production (i.e., inconsistent phonological errors) who may be resistant to more traditional therapy approaches.
Words selected for practice are those used frequently in the child’s functional communication. A list of frequently used words is developed (e.g., based on observation, parent report, and/or teacher report), and a number of words from this list are selected each week for treatment. The child is taught their “best” word production, and the words are practiced until consistently produced (Dodd et al., 2006). This approach is typically used before phonological contrast approaches.
Cycles Approach
The cycles approach combines target selection strategies and intervention schedule. The cycles approach targets phonological pattern errors and is designed for children with highly unintelligible speech who have extensive omissions, some substitutions, and a restricted use of consonants.
Treatment is scheduled in cycles, ranging from 5 to 16 weeks. During each cycle, one or more phonological patterns are targeted. After each cycle has been completed, another cycle begins, targeting one or more different phonological patterns. Recycling of phonological patterns continues until the targeted patterns are present in the child’s spontaneous speech (Hodson, 2010; Prezas & Hodson, 2010; Prezas et al., 2023).
The goal is to approximate the gradual typical phonological development process. There is no predetermined level of mastery of phonemes or phoneme patterns within each cycle; cycles are used to stimulate the emergence of a specific sound or pattern, not to produce mastery of it. Cycles can be used with multilingual learners (Prezas et al., 2023).
Integrated Phonological Awareness
Integrated phonological awareness is designed to improve a child’s representation of the sound structure of spoken language. Phoneme awareness tasks, combined with letter–sound knowledge, are incorporated into speech sound production intervention. Skills targeted in integrated phonological awareness might include rhyme, phoneme manipulation, phoneme identity, phoneme segmentation, phoneme blending, and linking speech to print (Gillon, 2000).
Metaphon Therapy
Metaphon therapy is designed to teach metaphonological awareness, or the awareness of the phonological structure of language. This approach assumes that children with phonological disorders have failed to acquire the rules of the phonological system.
The focus is on sound properties that need to be contrasted. For example, for problems with voicing, the concept of “noisy” (voiced) versus “quiet” (voiceless) is taught. Targets typically include processes that affect intelligibility, can be imitated, or are not seen in typically developing children of the same age (Dean et al., 1995; Howell & Dean, 1994).
Naturalistic Speech Intelligibility Intervention
Naturalistic speech intelligibility intervention addresses the targeted sound in naturalistic activities that provide the child with frequent opportunities for the sound to occur. For example, using a restaurant menu, signs at the grocery store, or favorite books, the child can be asked questions about words that contain the targeted sound(s). The child’s error productions are recast without the use of imitative prompts or direct motor training. This approach is used with children who can use the recasts effectively (Camarata, 2010).
Phonological Contrast Approaches
Phonological contrast approaches are frequently used to address phonological error patterns. They focus on improving phonemic contrasts in the child’s speech by emphasizing sound contrasts necessary to differentiate one word from another. Contrast approaches use contrasting word pairs as targets instead of individual sounds.
There are four different contrastive approaches:
- Minimal oppositions (also known as “minimal pairs” therapy)—uses pairs of words that differ by only one phoneme or single feature signaling a change in meaning. Minimal pairs are used to help establish contrasts not present in the child’s phonological system (e.g., /doʊɹ/ /soʊɹ/, /pɑt/ vs. /spɑt/, /ki/ vs. /ti/; Blache et al., 1981; Weiner, 1981). Children with a few speech errors may benefit the most from this approach (Storkel, 2022).
- Maximal oppositions—uses pairs of words containing a contrastive sound that is maximally distinct and varies on multiple dimensions (e.g., voice, place, and manner) to teach an unknown sound. For example, /mɑl/ and /kɑl/ are maximal pairs because /m/ is a bilabial voiced nasal, whereas /k/ is a velar voiceless stop (Gierut, 1989, 1990, 1992). Maximal oppositions may help children with several errors across different sound classes (Storkel, 2022). See Roth and Worthington’s (2018) Place, Manner, and Voicing Chart for English Consonants [PDF].
- Treatment of the empty set—similar to the maximal oppositions approach but uses pairs of words containing two maximally opposing sounds (e.g., /ɹ/ and /d/) that are unknown to the child (e.g., “row” vs. “doe” or “ray” vs. “day”; Gierut, 1992).
- Multiple oppositions—a variation of the minimal oppositions approach but uses pairs of words to target phoneme collapse (Storkel, 2022). Phoneme collapse happens when one sound substitutes many sounds, such as /d/ for /d, f, tʃ, s, t, st/. With multiple oppositions, the clinician could pair “door,” “four,” “chore,” “sore,” “tore,” and “store,” if /d/ is produced for targets /d, f, tʃ, s, t, st/.
Speech Motor Chaining
Speech motor chaining, based on motor learning theories, focuses on the repeated motor practice of speech targets (Preston et al., 2019). Sessions are divided into three phases. The first phase—prepractice or elicitation—focuses on the child distinguishing between the correct and incorrect productions of speech sounds. Once the child meets the criteria, the child moves onto the second phase, which is structured practice using speech motor chaining.
In the second phase, the child practices the target speech sound in the following progression:
- syllables
- monosyllabic words
- multisyllabic words
- phrases
- self-generated sentences
The child then transitions to the third phase—randomized practice—to vary stimuli and aid in learning. For additional information, see, for example, Preston et al. (2019).
Speech Sound Perception Training
Speech sound perception training is used to help a child acquire a stable perceptual representation for the target phoneme or phonological structure. The goal is to ensure that the child is attending to appropriate acoustic cues and weighing them according to a language-specific strategy (i.e., one that ensures reliable perception of the target in a variety of listening contexts). Potential contexts for speech perception training include the following (Cabbage & Hitchcock, 2022):
- stimulus type—natural speech versus synthetic speech
- perception type—between speakers versus within speaker
- task type—identification, discrimination, and being able to judge the accuracy of the speech sound
Examples of tasks are as follows:
- Auditory bombardment—Many and varied target exemplars are presented to the child, sometimes in a meaningful context such as a story and often with amplification.
- Identification tasks—The child identifies correct and incorrect versions of the target (e.g., /ræt/ is a correct exemplar of the word “rat,” whereas /wæt/ is not).
Tasks typically progress from the child judging speech produced by others to the child judging the accuracy of their own speech. Speech sound perception training is often used before and/or in conjunction with speech production training approaches. See Rvachew (1994), Rvachew et al. (1999, 2004), and Wolfe et al. (2003).
Treatment Techniques and Technologies
Techniques used in therapy to increase awareness of the target sound and/or provide feedback about placement and movement of the articulators include the following:
- Using a mirror for visual feedback of place and movement of articulators.
- Using gestural cueing for place or manner of production (e.g., using a long sweeping hand gesture for fricatives vs. a short “chopping” gesture for stops).
- Using ultrasound imaging (placement of an ultrasound transducer under the chin) as a biofeedback technique to visualize tongue position and configuration (Adler-Bock et al., 2007; S. A. S. Lee et al., 2015; Preston et al., 2013, 2014).
- Using palatography (various coloring agents or a palatal device with electrodes) to record and visualize contact of the tongue on the palate while the child makes different speech sounds (Dagenais, 1995; Gibbon et al., 1999; Hitchcock et al., 2017).
- Amplifying target sounds to improve attention, reduce distractibility, and increase sound awareness and discrimination—for example, auditory bombardment with low-level amplification is used with the cycles approach at the beginning and end of each session to help children perceive differences between errors and target sounds (Hodson, 2010).
- Providing spectral biofeedback through a visual representation of the acoustic signal of speech (McAllister Byun & Hitchcock, 2012).
- Providing tactile biofeedback using tools, devices, or substances placed within the mouth (e.g., tongue depressors, peanut butter) to provide feedback on correct tongue placement and coordination (Altshuler, 1961; Leonti et al., 1975; Shriberg, 1980).
Nonspeech oral motor exercises involve the use of oral motor training prior to teaching sounds or as a supplement to speech sound instruction. SLPs carefully consider what a particular oral motor activity is likely to accomplish and whether it addresses the child’s speech sound error (McCauley et al., 2009). Systematic reviews of nonspeech oral motor therapy for children with SSDs provide more information to help guide decision making (see, e.g., A. S.-Y. Lee & Gibbon, 2015; McCauley et al., 2009). See also the Treatment section of the Speech Sound Disorders Evidence Map filtered for Oral–Motor Exercises.
Considerations for Treating Multilingual or Multidialectal Populations
When treating a multilingual or multidialectal individual with an SSD, the clinician works with multiple sound systems. Although there may be some overlap in the phonemic inventories, there will be some sounds unique to each language and different rules for each linguistic system. One linguistic sound system may influence production in the other sound system.
Strategies used when designing a treatment protocol include
- determining whether to use a multilingual, multidialectal, or cross-linguistic approach (see ASHA’s Practice Portal page on Multilingual Service Delivery in Audiology and Speech-Language Pathology);
- selecting targets based on shared versus unshared sounds;
- using intervention approaches that implement a combination of multilingual and cross-linguistic approaches as well as a balanced combination of earlier and later developing sounds following Vygotsky’s zone of proximal development (e.g., multilingual cycles approach; Prezas, 2025; Prezas et al., 2023);
- determining how language(s) and dialect(s) will be used in services, on the basis of factors such as language history, language use, and communicative needs;
- understanding the influence of the rules of the communication profile that may influence speech sound production;
- identifying alternative means of providing accurate models for target phonemes that are unique to the child’s language, when the clinician is unable to do so; and
- noting if success generalizes across languages throughout the treatment process (Goldstein & Fabiano, 2007).
Considerations for Treatment in Schools
Determining eligibility for services in a school setting is detailed in the Individuals with Disabilities Education Improvement Act of 2004 (IDEA). In accordance with this regulation, the SLP determines
- if a child has an SSD in all languages or dialects used,
- if there is an adverse effect on educational performance or social interactions resulting from the disability,
- if the child meets eligibility criteria specific to that state, and
- if specially designed instruction and/or related services and supports are needed to help the child make progress in the general education curriculum.
Examples of adverse effects on educational performance and social interactions are as follows:
- The SSD affects the child’s ability or willingness to communicate in the classroom (e.g., responding to teachers’ questions, participating in classroom discussions) and to interact in social settings with peers (e.g., interactions during lunch and recess; Krueger, 2019).
- The SSD may co-occur with difficulties in phonological skills that affect spelling, reading, and writing (Farquharson & Boldini, 2018; Ireland et al., 2020). For example, the way a child spells a word reflects the errors made when the word is spoken.
See ASHA’s resource on language in brief and ASHA’s Practice Portal pages on Spoken Language Disorders and Written Language Disorders for more information about the relationship between spoken and written language.
For more information about eligibility for services in the schools, see ASHA’s resources on eligibility and dismissal in schools, IDEA Part B: Individualized Education Programs and Eligibility for Services, and Current IDEA Part C Final Regulations (2011).
If a child is not eligible for services under the IDEA, they may still be eligible to receive services under the Rehabilitation Act of 1973, Section 504 [PDF]. See ASHA’s Practice Portal page on Documentation in Schools for more information about Section 504 of the Rehabilitation Act of 1973.
Children With Persisting Speech Difficulties
Speech difficulties sometimes persist throughout the school years and into adulthood. Pascoe et al. (2006) define persisting speech difficulties as “difficulties in the normal development of speech that do not resolve as the child matures or even after they receive specific help for these problems” (p. 2). The population of people with persisting speech difficulties is diverse in terms of etiology, severity, and the nature of speech difficulties (Dodd, 2005; Shriberg et al., 2010; Stackhouse, 2006; Wren et al., 2012).
A person with persisting speech difficulties may be at risk for
- difficulty communicating effectively when speaking,
- difficulty acquiring reading and writing skills (Farquharson et al., 2018, 2021), and
- psychosocial problems (e.g., low self-esteem, increased risk of bullying; see, e.g., McCormack et al., 2012).
Intervention approaches vary and may depend on the person’s area(s) of difficulty (e.g., spoken language, written language, and/or psychosocial issues).
In designing an effective treatment protocol, the SLP considers
- teaching and encouraging the use of self-monitoring strategies to facilitate consistent use of learned skills;
- educating and coaching parents;
- collaborating with teachers and other school personnel to support the student and to facilitate their access to the academic curriculum; and
- managing psychosocial factors, including self-esteem issues and bullying (Pascoe et al., 2006).
Postsecondary Transition Planning
Children with persisting speech difficulties may continue to have problems with oral communication, reading and writing, and social aspects of life as they transition to postsecondary education and vocational settings (Carrigg et al., 2015; Hitchcock et al., 2015). The potential impact of persistent speech difficulties highlights the need for continued support to facilitate a successful transition to young adulthood. For more information about transition planning, see ASHA’s resource on postsecondary transition planning.
Service Delivery
See the Service Delivery section of the Speech Sound Disorders Evidence Map for pertinent scientific evidence, expert opinion, and client/caregiver perspective.
In addition to determining the type of speech and language treatment that is optimal for children with SSDs, SLPs consider other service delivery variables that may have an impact on treatment outcomes, including dosage and format. For more information, see ASHA’s resource on school-based service delivery in speech-language pathology.
ASHA Resources
- Assessment Tools, Techniques, and Data Sources
- Consumer Information: Speech Sound Disorders
- Current IDEA Part C Final Regulations (2011)
- Eligibility and Dismissal in Schools
- Focusing on Care on Individuals and Their Care Partners
- IDEA Part B: Individualized Education Programs and Eligibility for Services
- Interprofessional Education/Interprofessional Practice (IPE/IPP)
- Language In Brief
- Let's Talk: For People With Special Communication Needs
- Person-Centered Focus on Function: Speech Sound Disorder [PDF]
- Phonemic Inventories and Cultural and Linguistic Information Across Languages
- Postsecondary Transition Planning
- Response to Intervention
- School-Based Service Delivery in Speech-Language Pathology
- Selected Phonological Patterns
- Social Determinants of Health
- Speech Characteristics: Selected Populations [PDF]
Other Resources
This list of resources is not exhaustive, and the inclusion of any specific resource does not imply endorsement from ASHA.
- Adventures in Speech Pathology | Free Resources for the Multiple Oppositions Approach
- American Cleft Palate Craniofacial Association
- Consonant Age of Acquisition (Crowe & McLeod, 2020) [PDF]
- Everyone Has an Accent
- Multilingual Children's Speech: Overview
- Multilingual Children's Speech: Intelligibility in Context Scale (ICS)
- Multilingual Children's Speech: Speech Participation and Activity Assessment of Children (SPAA-C)
- Phonetics: The Sounds of American English (University of Iowa)
- Phonological Development Tools and Cross-linguistic Phonology Project (The University of British Columbia)
- Place, Manner, and Voicing Chart for English Consonants (Roth & Worthington, 2018) [PDF]
- RCSLT: New Long COVID Guidance and Patient Handbook
- Reading Rockets | Target the Problem: Phonological and Phonemic Awareness
- Reading Rockets | The Development of Phonological Skills (WETA Educational Website)
- The Speech Accent Archive (George Mason University)
Adler-Bock, M., Bernhardt, B. M., Gick, B., & Bacsfalvi, P. (2007). The use of ultrasound in remediation of North American English /r/ in 2 adolescents. American Journal of Speech-Language Pathology, 16(2), 128–139. https://doi.org/10.1044/1058-0360(2007/017)
Altshuler, M. W. (1961). A therapeutic oral device for lateral emission. Journal of Speech and Hearing Disorders, 26(2), 179–181. https://doi.org/10.1044/jshd.2602.179
American Speech-Language-Hearing Association. (2016). Scope of practice in speech-language-pathology [Scope of practice]. https://www.asha.org/policy/
American Speech-Language-Hearing Association. (2023). Code of ethics [Ethics]. https://www.asha.org/policy/
Anthony, J. L., Aghara, R. G., Dunkelberger, M. J., Anthony, T. I., Williams, J. M., & Zhang, Z. (2011). What factors place children with speech sound disorders at risk for reading problems? American Journal of Speech-Language Pathology, 20(2), 146–160. https://doi.org/10.1044/1058-0360(2011/10-0053)
Baker, E., & Williams, A. L. (2010). Complexity approaches to intervention. In S. F. Warren & M. E. Fey (Series Eds.). & A. L. Williams, S. McLeod, & R. J. McCauley (Volume Eds.), Intervention for speech sound disorders in children (pp. 95–115). Baltimore, MD: Brookes.
Bernthal, J. E., Bankson, N. W., & Flipsen, P., Jr. (2022). Speech sound disorders in children: Articulation & phonological disorders (9th ed). Brookes Publishing.
Blache, S. E., Parsons, C. L., & Humphreys, J. M. (1981). A minimal-word-pair model for teaching the linguistic significant difference of distinctive feature properties. Journal of Speech and Hearing Disorders, 46(3), 291–296. https://doi.org/10.1044/jshd.4603.291
Bleile, K. (2002). Evaluating articulation and phonological disorders when the clock is running. American Journal of Speech-Language Pathology, 11(3), 243–249. https://doi.org/10.1044/1058-0360(2002/026)
Brown, B. B., Bendersky, M., & Chapman, T. (1986). The early utterances of preterm infants. British Journal of Disorders of Communication, 21(3), 307–320. https://doi.org/10.3109/13682828609019844
Bruce, L., Lynde, S., Weinhold, J., & Peter, B. (2018). A team approach to response to intervention for speech sound errors in the school setting. Perspectives of the ASHA Special Interest Groups, 3(16), 110–119. https://doi.org/10.1044/persp3.SIG16.110
Cabbage, K. L., & Hitchcock, E. R. (2022). Clinical considerations for speech perception in school-age children with speech sound disorders: A review of the current literature. Language, Speech, and Hearing Services in Schools, 53(3), 768–785. https://doi.org/10.1044/2022_LSHSS-21-00120
Cabbage, K. L. (2015). The role of speech perception in persistent speech sound disorder. Perspectives on School-Based Issues, 16(2), 18–24. https://doi.org/10.1044/sbi16.2.18
Camarata, S. (2010). Naturalistic intervention for speech intelligibility and speech accuracy. In A. L. Williams, S. McLeod, & R. J. McCauley (Eds.), Interventions for speech sound disorders in children (pp. 381–406). Brookes.
Campbell, T. F., Dollaghan, C. A., Rockette, H. E., Paradise, J. L., Feldman, H. M., Shriberg, L. D., Sabo, D. L., & Kurs-Lasky, M. (2003). Risk factors for speech delay of unknown origin in 3-year-old children. Child Development, 74(2), 346–357. https://doi.org/10.1111/1467-8624.7402002
Carrigg, B., Baker, E., Parry, L., & Ballard, K. J. (2015). Persistent speech sound disorder in a 22-year-old male: Communication, educational, socio-emotional, and vocational outcomes. Perspectives on School-Based Issues, 16(2), 37–49. https://doi.org/10.1044/sbi16.2.37
Carroll, J. M., Snowling, M. J., Stevenson, J., & Hulme, C. (2003). The development of phonological awareness in preschool children. Developmental Psychology, 39(5), 913–923. https://doi.org/10.1037/0012-1649.39.5.913
Catts, H. W., McIlraith, A., Bridges, M. S., & Nielsen, D. C. (2017). Viewing a phonological deficit within a multifactorial model of dyslexia. Reading and Writing, 30, 613–629. https://doi.org/10.1007/s11145-016-9692-2
Celce-Murcia, M., Brinton, D. M., & Goodwin, J. M. (1996). Teaching pronunciation: A reference for teachers of English to speakers of other languages. Cambridge University Press.
Center on Multi-Tiered System of Supports. (n.d.). Essential components of MTSS. https://mtss4success.org/essential-components
Coplan, J., & Gleason, J. R. (1988). Unclear speech: Recognition and significance of unintelligible speech in preschool children. Pediatrics, 82(3), 447–452.
Crowe, K., & McLeod, S. (2020). Children’s English consonant acquisition in the United States: A review. American Journal of Speech-Language
Pathology, 29(4), 2155–2169. https://doi.org/10.1044/2020_AJSLP-19-00168
Dagenais, P. A. (1995). Electropalatography in the treatment of articulation/phonological disorders. Journal of Communication Disorders, 28(4), 303–329. https://doi.org/10.1016/0021-9924(95)00059-1
Dean, E. C., Howell, J., Waters, D., & Reid, J. (1995). Metaphon: A metalinguistic approach to the treatment of phonological disorder in children. Clinical Linguistics & Phonetics, 9(1), 1–19. https://doi.org/10.3109/02699209508985318
Dodd, B. (2005). Differential diagnosis and treatment of children with speech disorder. Whurr.
Dodd, B., Holm, A., Crosbie, S., & McIntosh, B. (2006). A core vocabulary approach for management of inconsistent speech disorder. Advances in Speech Language Pathology, 8(3), 220–230. https://doi.org/10.1080/14417040600738177
Eadie, P., Morgan, A., Ukoumunne, O. C., Eecen, K. T., Wake, M., & Reilly, S. (2015). Speech sound disorder at 4 years: Prevalence, comorbidities, and predictors in a community cohort of children. Developmental Medicine & Child Neurology, 57(6), 578–584. https://doi.org/10.1111/dmcn.12635
Ertmer, D. J. (2010). Relationships between speech intelligibility and word articulation scores in children with hearing loss. Journal of Speech, Language, and Hearing Research, 53(5), 1075–1086. https://doi.org/10.1044/1092-4388(2010/09-0250)
Everhart, R. W. (1960). Literature survey of growth and developmental factors in articulatory maturation. Journal of Speech and Hearing Disorders, 25(1), 59–69. https://doi.org/10.1044/jshd.2501.59
Fabiano-Smith, L. (2019). Standardized tests and the diagnosis of speech sound disorders. Perspectives of the ASHA Special Interest Groups, 4(1), 58–66. https://doi.org/10.1044/2018_PERS-SIG1-2018-0018
Farquharson, K. (2019). It might not be “just artic”: The case for the single sound error. Perspectives of the ASHA Special Interest Groups, 4(1), 76–84. https://doi.org/10.1044/2018_PERS-SIG1-2018-0019
Farquharson, K., & Boldini, L. (2018). Variability in interpreting “educational performance” for children with speech sound disorders. Language, Speech, and Hearing Services in Schools, 49(4), 938–949. https://doi.org/10.1044/2018_LSHSS-17-0159
Farquharson, K., Hogan, T. P., & Bernthal, J. E. (2018). Working memory in school-age children with and without a persistent speech sound disorder. International Journal of Speech-Language Pathology, 20(4), 422–433. https://doi.org/10.1080/17549507.2017.1293159
Farquharson, K., Hogan, T. P., & Fox, A. B. (2021). Factors that influence non‐word repetition performance in children with and without persistent speech sound disorders. International Journal of Language & Communication Disorders, 56(6), 1218–1234. https://doi.org/10.1111/1460-6984.12663
Felsenfeld, S., McGue, M., & Broen, P. A. (1995). Familial aggregation of phonological disorders: Results from a 28-year follow-up. Journal of Speech and Hearing Research, 38(5), 1091–1107. https://doi.org/10.1044/jshr.3805.1091
Fey, M. (1986). Language intervention with young children. Allyn & Bacon.
Flipsen, P., Jr. (2006). Measuring the intelligibility of conversational speech in children. Clinical Linguistics & Phonetics, 20(4), 202–312. https://doi.org/10.1080/02699200400024863
Flipsen, P., Jr. (2015). Emergence and prevalence of persistent and residual speech errors. Seminars in Speech and Language, 36(04), 217–223. https://doi.org/10.1055/s-0035-1562905
Flipsen, P., Jr., & Sacks, S. (2022). The SATPAC approach and remediation of speech sound errors in an RTI context: A replication. Perspectives of the ASHA Special Interest Groups, 7(3), 912– 925. https://doi.org/10.1044/2022_PERSP-21-00320
Fox, A. V., Dodd, B., & Howard, D. (2002). Risk factors for speech disorders in children. International Journal of Language & Communication Disorders, 37(2), 117–132. https://doi.org/10.1080/13682820110116776
Gibbon, F., Stewart, F., Hardcastle, W. J., & Crampin, L. (1999). Widening access to electropalatography for children with persistent sound system disorders. American Journal of Speech-Language Pathology, 8(4), 319–333. https://doi.org/10.1044/1058-0360.0804.319
Gierut, J. A. (1989). Maximal opposition approach to phonological treatment. Journal of Speech and Hearing Disorders, 54(1), 9–19. https://doi.org/10.1044/jshd.5401.09
Gierut, J. A. (1990). Differential learning of phonological oppositions. Journal of Speech and Hearing Research, 33(3), 540–549. https://doi.org/10.1044/jshr.3303.540
Gierut, J. A. (1992). The conditions and course of clinically induced phonological change. Journal of Speech and Hearing Research, 35(5), 1049–1063. https://doi.org/10.1044/jshr.3505.1049
Gierut, J. A. (2007). Phonological complexity and language learnability. American Journal of Speech-Language Pathology, 16(1), 6–17. https://doi.org/10.1044/1058-0360(2007/003)
Gillon, G. T. (2000). The efficacy of phonological awareness intervention for children with spoken language impairment. Language, Speech, and Hearing Services in Schools, 31(2), 126–141. https://doi.org/10.1044/0161-1461.3102.126
Glaspey, A., & Stoel-Gammon, C. (2007). A dynamic approach to phonological assessment. Advances in Speech Language Pathology, 9(4), 286–296. https://doi.org/10.1080/14417040701435418
Goldstein, B. A., & Fabiano, L. (2007). Assessment and intervention for bilingual children with phonological disorders. The ASHA Leader, 12(2), 6–31. https://doi.org/10.1044/leader.FTR2.12022007.6
Grunwell, P. (1987). Clinical phonology (2nd ed.). Chapman & Hall.
Hayiou-Thomas, M. E., Carroll, J. M., Leavett, R., Hulme, C., & Snowling, M. J. (2017). When does speech sound disorder matter for literacy? The role of disordered speech errors, co-occurring language impairment and family risk of dyslexia. The Journal of Child Psychology and Psychiatry, 58(2), 197–205. https://doi.org/10.1111/jcpp.12648
Hearnshaw, S., Baker, E., & Munro, N. (2019). Speech perception skills of children with speech sound disorders: A systematic review and meta-analysis. Journal of Speech, Language, and Hearing Research, 62(10), 3771–3789. https://doi.org/10.1044/2019_JSLHR-S-18-0519
Hitchcock, E. R., Harel, D., & McAllister Byun, T. (2015). Social, emotional, and academic impact of residual speech errors in school-aged children: A survey study. Seminars in Speech and Language, 36(4), 283–294. https://doi.org/10.1055/s-0035-1562911
Hitchcock, E. R., McAllister Byun, T., Swartz, M., & Lazarus, R. (2017). Efficacy of electropalatography for treating misarticulation of /r/. American Journal of Speech-Language Pathology, 26(4), 1141–1158. https://doi.org/10.1044/2017_AJSLP-16-0122
Hodson, B. W. (2010). Evaluating and enhancing children’s phonological systems: Research and theory to practice. PhonoComp Publishing.
Howell, J., & Dean, E. (1994). Treating phonological disorders in children: Metaphon—Theory to practice (2nd ed.). Whurr.
Hustad, K. C., Mahr, T. J., Natzke, P., & Rathouz, P. J. (2021). Speech development between 30 and 119 months in typical children I: Intelligibility growth curves for single-word and multiword productions. Journal of Speech, Language, and Hearing Research, 64(10), 3707– 3719. https://doi.org/10.1044/2021_JSLHR-21-00142
Individuals with Disabilities Education Improvement Act of 2004, Pub. L. No. 108-446, 20 U.S.C. § 1400 et seq. (2004). http://idea.ed.gov/
Ireland, M., McLeod, S., Farquharson, K., & Crowe, K. (2020). Evaluating children in U.S. public schools with speech sound disorders: Considering federal and state laws, guidance, and research. Topics in Language Disorders, 40(4), 326–340. https://doi.org/10.1097/TLD.0000000000000226
Jessup, B., Ward, E., Cahill, L., & Keating, D. (2008). Prevalence of speech and/or language impairment in preparatory students in northern Tasmania. International Journal of Speech-Language Pathology, 10(5), 364–377. https://doi.org/10.1080/17549500701871171
Kent, R. D., Miolo, G., & Bloedel, S. (1994). The intelligibility of children’s speech: A review of evaluation procedures. American Journal of Speech-Language Pathology, 3(2), 81–95. https://doi.org/10.1044/1058-0360.0302.81
Krueger, B. I. (2019). Eligibility and speech sound disorders: Assessment of social impact. Perspectives of the ASHA Special Interest Groups, 4(1), 85–90. https://doi.org/10.1044/2018_PERS-SIG1-2018-0016
Lee, A. S.-Y., & Gibbon, F. E. (2015). Non-speech oral motor treatment for children with developmental speech sound disorders. Cochrane Database of Systematic Reviews, 2015(3), 1–42. https://doi.org/10.1002/14651858.CD009383.pub2
Lee, S. A. S., Wrench, A., & Sancibrian, S. (2015). How to get started with ultrasound technology for treatment of speech sound disorders. Perspectives on Speech Science and Orofacial Disorders, 25(2), 66–80. https://doi.org/10.1044/ssod25.2.66
Leitão, S., & Fletcher, J. (2004). Literacy outcomes for students with speech impairment: Long-term follow-up. International Journal of Language & Communication Disorders, 39(2), 245–256. https://doi.org/10.1080/13682820310001619478
Leonti, S., Blakeley, R., & Louis, H. (1975, November). Spontaneous correction of resistant /ɚ/ and /r/ using an oral prosthesis [Paper presentation]. American Speech and Hearing Association Convention, Washington, DC, United States.
Lewis, B. A., Avrich, A. A., Freebairn, L. A., Hansen, A. J., Sucheston, L. E., Kuo, I., Taylor, H. G., Iyengar, S. K., & Stein, C. M. (2011). Literacy outcomes of children with early childhood speech sound disorders: Impact of endophenotypes. Journal of Speech, Language, and Hearing Research, 54(6), 1628–1643. https://doi.org/10.1044/1092-4388(2011/10-0124)
Locke, J. L. (1980). The inference of speech perception in the phonologically disordered child. Part I: A rationale, some criteria, the conventional tests. Journal of Speech and Hearing Disorders, 45(4), 431–444. https://doi.org/10.1044/jshd.4504.431
McAllister Byun, T., & Hitchcock, E. R. (2012). Investigating the use of traditional and spectral biofeedback approaches to intervention for /r/ misarticulation. American Journal of Speech-Language Pathology, 21(3), 207–221. https://doi.org/10.1044/1058-0360(2012/11-0083)
McCauley, R. J., Strand, E., Lof, G. L., Schooling, T., & Frymark, T. (2009). Evidence-based systematic review: Effects of nonspeech oral motor exercises on speech. American Journal of Speech-Language Pathology, 18(4), 343–360. https://doi.org/10.1044/1058-0360(2009/09-0006)
McCormack, J., McAllister, L., McLeod, S., & Harrison, L. (2012). Knowing, having, doing: The battles of childhood speech impairment. Child Language Teaching and Therapy, 28(2), 141–157. https://doi.org/10.1177/0265659011417313
McDonald, E. T. (1974). Articulation testing and treatment: A sensory motor approach. Stanwix House.
McKinnon, D. H., McLeod, S., & Reilly, S. (2007). The prevalence of stuttering, voice, and speech-sound disorders in primary school students in Australia. Language, Speech, and Hearing Services in Schools, 38(1), 5–15. https://doi.org/10.1044/0161-1461(2007/002)
McLeod, S., Harrison, L. J., & McCormack, J. (2012). The Intelligibility in Context Scale: Validity and reliability of a subjective rating measure. Journal of Speech, Language, and Hearing Research, 55(2), 648–656. https://doi.org/10.1044/1092-4388(2011/10-0130)
McLeod, S., Verdon, S., & The International Expert Panel on Multilingual Children’s Speech. (2017). Tutorial: Speech assessment for multilingual children who do not speak the same language(s) as the speech-language pathologist. American Journal of Speech-Language Pathology, 26(3), 691–708. https://doi.org/10.1044/2017_AJSLP-15-0161
McNeill, B. C., & Hesketh, A. (2010). Developmental complexity of the stimuli included in mispronunciation detection tasks. International Journal of Language & Communication Disorders, 45(1), 72–82. https://doi.org/10.3109/13682820902745479
Morley, D. E. (1952). A ten-year survey of speech disorders among university students. Journal of Speech and Hearing Disorders, 17(1), 25–31. https://doi.org/10.1044/jshd.1701.25
Mullen, R., & Schooling, T. (2010). The National Outcomes Measurement System for pediatric speech-language pathology. Language, Speech, and Hearing Services in Schools, 41(1), 44–60. https://doi.org/10.1044/0161-1461(2009/08-0051)
Murray, E., Iuzzini-Seigel, J., Maas, E., Terband, H., & Ballard, K. J. (2021). Differential diagnosis of childhood apraxia of speech compared to other speech sound disorders: A systematic review. American Journal of Speech-Language Pathology, 30(1), 279–300. https://doi.org/10.1044/2020_AJSLP-20-00063
National Institute for Literacy. (2009). Developing early literacy: Report of the National Early Literacy Panel. A scientific synthesis of early literacy development and implications for intervention. U.S. Department of Education.
Office of Special Education and Rehabilitative Services. (2011). A response to intervention (RTI) process cannot be used to delay-deny an evaluation for eligibility under the Individuals with Disabilities Education Act (IDEA) (OSEP Memo 11-07). U.S. Department of Education. https://sites.ed.gov/idea/idea-files/osep-memo-11-07-response-to-intervention-rti-memo/
Overby, M. S., Trainin, G., Smit, A. B., Bernthal, J. E., & Nelson, R. (2012). Preliteracy speech sound production skill and later literacy outcomes: A study using the Templin Archive. Language, Speech, and Hearing Services in Schools, 43(1), 97–115. https://doi.org/10.1044/0161-1461(2011/10-0064)
Pascoe, M., Stackhouse, J., & Wells, B. (2006). Persisting speech difficulties in children: Children’s speech and literacy difficulties, Book 3. Whurr.
Pearson, B. Z., Velleman, S. L., Bryant, T. J., & Charko, T. (2009). Phonological milestones for African American English–speaking children learning Mainstream American English as a second dialect. Language, Speech, and Hearing Services in Schools, 40(3), 229–244. https://doi.org/10.1044/0161-1461(2008/08-0064)
Peña-Brooks, A., & Hegde, M. N. (2023). Assessment and treatment of articulation and phonological disorders in children (4th ed.). Pro-Ed.
Peterson, R. L., Pennington, B. F., Shriberg, L. D., & Boada, R. (2009). What influences literacy outcome in children with speech sound disorder? Journal of Speech, Language, and Hearing Research, 52(5), 1175–1188. https://doi.org/10.1044/1092-4388(2009/08-0024)
Powell, T. W., & Miccio, A. W. (1996). Stimulability: A useful clinical tool. Journal of Communication Disorders, 29(4), 237–253. https://doi.org/10.1016/0021-9924(96)00012-3
Preston, J. L., Brick, N., & Landi, N. (2013). Ultrasound biofeedback treatment for persisting childhood apraxia of speech. American Journal of Speech-Language Pathology, 22(4), 627–643. https://doi.org/10.1044/1058-0360(2013/12-0139)
Preston, J. L., Leece, M. C., & Storto, J. (2019). Tutorial: Speech motor chaining treatment for school-age children with speech sound disorders. Language, Speech, and Hearing Services in Schools, 50(3), 343–355. https://doi.org/10.1044/2018_LSHSS-18-0081
Preston, J. L., McCabe, P., Rivera-Campos, A., Whittle, J. L., Landry, E., & Maas, E. (2014). Ultrasound visual feedback treatment and practice variability for residual speech sound errors. Journal of Speech, Language, and Hearing Research, 57(6), 2102–2115. https://doi.org/10.1044/2014_JSLHR-S-14-0031
Prezas, R. (2025). Using the cycles approach to enhance multilingual children’s phonological systems. In B. W. Hodson, Evaluating and enhancing children’s phonological systems: Research and theory to practice (2nd ed.). PhonoComp Publishing.
Prezas, R. F., & Hodson, B. W. (2010). The cycles phonological remediation approach. In A. L. Williams, S. McLeod, & R. J. McCauley (Eds.), Interventions for speech sound disorders in children (pp. 137–158). Brookes.
Prezas, R. F., Magnus, L. C., & Hodson, B. W. (2023). The cycles phonological pattern approach: Expediting intelligibility. In C. Bowen, Children’s speech sound disorders (3rd ed., pp. 41–47). Wiley.
Roepke, E. (2024). Assessing phonological processing in children with speech sound disorders. Perspectives of the ASHA Special Interest Groups, 9(1), 14–34. https://doi.org/10.1044/2023_PERSP-23-00036
Roth, F. P., & Worthington, C. K. (2018). Treatment resource manual for speech-language pathology. Plural.
Rvachew, S. (1994). Speech perception training can facilitate sound production learning. Journal of Speech and Hearing Research, 37(2), 347–357. https://doi.org/10.1044/jshr.3702.347
Rvachew, S., & Bernhardt, B. M. (2010). Clinical implications of dynamic systems theory for phonological development. American Journal of Speech-Language Pathology, 19(1), 34–50. https://doi.org/10.1044/1058-0360(2009/08-0047)
Rvachew, S., & Matthews, T. (2024). Considerations for identifying subtypes of speech sound disorder. International Journal of Language & Communication Disorders, 59(6), 2146–2157. https://doi.org/10.1111/1460-6984.13108
Rvachew, S., Nowak, M., & Cloutier, G. (2004). Effect of phonemic perception training on the speech production and phonological awareness skills of children with expressive phonological delay. American Journal of Speech-Language Pathology, 13(3), 250–263. https://doi.org/10.1044/1058-0360(2004/026)
Rvachew, S., Rafaat, S., & Martin, M. (1999). Stimulability, speech perception skills, and the treatment of phonological disorders. American Journal of Speech-Language Pathology, 8(1), 33–43. https://doi.org/10.1044/1058-0360.0801.33
Section 504 of the Rehabilitation Act of 1973, Pub. L. No. 93-112, 29 U.S.C. § 794.
Seeff-Gabriel, B., Chiat, S., & Dodd, B. (2010). Sentence imitation as a tool in identifying expressive morphosyntactic difficulties in children with severe speech difficulties. International Journal of Language & Communication Disorders, 45(6), 691–702. https://doi.org/10.3109/13682820903509432
Shollenbarger, A. J., Robinson, G. C., Taran, V., & Choi, S. (2017). How African American English–speaking first graders segment and rhyme words and nonwords with final consonant clusters. Language, Speech, and Hearing Services in Schools, 48(4), 273–285. https://doi.org/10.1044/2017_LSHSS-16-0062
Shriberg, L. D. (1980). An intervention procedure for children with persistent /r/ errors. Language, Speech, and Hearing Services in Schools, 11(2), 102–110. https://doi.org/10.1044/0161-1461.1102.102
Shriberg, L. D., & Austin, D. (1998). Comorbidity of speech-language disorders: Implications for a phenotype marker for speech delay. In R. Paul (Ed.), The speech-language connection (pp. 73–117). Brookes.
Shriberg, L. D., Austin, D., Lewis, B. A., McSweeny, J. L., & Wilson, D. L. (1997). The percentage of consonants correct (PCC) metric: Extensions and reliability data. Journal of Speech, Language, and Hearing Research, 40(4), 708–722. https://doi.org/10.1044/jslhr.4004.708
Shriberg, L. D., Fourakis, M., Hall, S. D., Karlsson, H. B., Lohmeier, H. L., McSweeny, J. L., Potter, N. L., Scheer-Cohen, A. R., Strand, E. A., Tilkens, C. M., & Wilson, D. L. (2010). Extensions to the Speech Disorders Classification System (SDCS). Clinical Linguistics & Phonetics, 24(10), 795–824. https://doi.org/10.3109/02699206.2010.503006
Shriberg, L. D., & Kwiatkowski, J. (1980). Natural process analysis (NPA): A procedure for phonological analysis of continuous speech samples. Macmillan.
Shriberg, L. D., & Kwiatkowski, J. (1982a). Phonological disorders II: A conceptual framework for management. Journal of Speech and Hearing Disorders, 47(3), 242–256. https://doi.org/10.1044/jshd.4703.242
Shriberg, L. D., & Kwiatkowski, J. (1982b). Phonological disorders III: A procedure for assessing severity of involvement. Journal of Speech and Hearing Disorders, 47(3), 256–270. https://doi.org/10.1044/jshd.4703.256
Shriberg, L. D., & Kwiatkowski, J. (1994). Developmental phonological disorders I: A clinical profile. Journal of Speech and Hearing Research, 37(5), 1100–1126. https://doi.org/10.1044/jshr.3705.1100
Shriberg, L. D., Tomblin, J. B., & McSweeny, J. L. (1999). Prevalence of speech delay in 6-year-old children and comorbidity with language impairment. Journal of Speech, Language, and Hearing Research, 42(6), 1461–1481. https://doi.org/10.1044/jslhr.4206.1461
Silva, P. A., Chalmers, D., & Stewart, I. (1986). Some audiological, psychological, educational and behavioral characteristics of children with bilateral otitis media with effusion: A longitudinal study. Journal of Learning Disabilities, 19(3), 165–169. https://doi.org/10.1177/002221948601900307
Stackhouse, J. (2006). Speech and spelling difficulties: Who is at risk and why? In M. Snowling & J. Stackhouse (Eds.), Dyslexia, speech and language: A practitioner’s handbook (pp. 15–35). Whurr.
Storkel, H. L. (2018). The complexity approach to phonological treatment: How to select treatment targets. Language, Speech, and Hearing Services in Schools, 49(3), 463–481. https://doi.org/10.1044/2017_LSHSS-17-0082
Storkel, H. L. (2022). Minimal, maximal, or multiple: Which contrastive intervention approach to use with children with speech sound disorders? Language, Speech, and Hearing Services in Schools, 53(3), 632–645. https://doi.org/10.1044/2021_LSHSS-21-00105
Strand, E. A., McCauley, R. J., Weigand, S. D., Stoeckel, R. E., & Baas, B. S. (2013). A motor speech assessment for children with severe speech disorders: Reliability and validity evidence. Journal of Speech, Language, and Hearing Research, 56(2), 505–520. https://doi.org/10.1044/1092-4388(2012/12-0094)
Swaminathan, D., & Farquharson, K. (2018). Using response to intervention for speech sound disorders: Exploring practice characteristics and geographical differences. Perspectives of the ASHA Special Interest Groups, 3(16), 53–66. https://doi.org/10.1044/persp3.SIG16.53
Sylvan, L. (2023). Overcoming the research–practice gap: Key considerations for speech-language pathologists related to multitiered systems of support. Perspectives of the ASHA Special Interest Groups, 8(6), 1–17. https://doi.org/10.1044/2023_PERSP-23-00103
Tambyraja, S. R., Farquharson, K., & Justice, L. (2020). Reading risk in children with speech sound disorder: Prevalence, persistence, and predictors. Journal of Speech, Language, and Hearing Research, 63(11), 3714–3726. https://doi.org/10.1044/2020_JSLHR-20-00108
Teele, D. W., Klein, J. O., Chase, C., Menyuk, P., Rosner, B. A., & the Greater Boston Otitis Media Study Group. (1990). Otitis media in infancy and intellectual ability, school achievement, speech, and language at age 7 years. The Journal of Infectious Diseases, 162(3), 685–694. https://www.jstor.org/stable/30131702
Tyler, A. A., & Tolbert, L. C. (2002). Speech-language assessment in the clinical setting. American Journal of Speech-Language Pathology, 11(3), 215–220. https://doi.org/10.1044/1058-0360(2002/022)
Unicomb, R., Kefalianos, E., Reilly, S., Cook, F., & Morgan, A. (2020). Prevalence and features of comorbid stuttering and speech sound disorder at age 4 years. Journal of Communication Disorders, 84, 105976. https://doi.org/10.1016/j.jcomdis.2020.105976
Valles, B., Jr. (2015). The impact of accented English on speech comprehension (Publication No. 3708574) [Doctoral dissertation, The University of Texas at El Paso]. ProQuest Dissertations and Theses—Gradworks. https://scholarworks.utep.edu/dissertations/AAI3708574/
Velleman, S. L., & Pearson, B. Z. (2010). Differentiating speech sound disorders from phonological dialect differences: Implications for assessment and intervention. Topics in Language Disorders, 30(3), 176–188. https://doi.org/10.1097/TLD.0b013e3181efc378
Wagner, R. K., & Torgesen, J. K. (1987). The nature of phonological processing and its causal role in the acquisition of reading skills. Psychological Bulletin, 101(2), 192–212. https://doi.org/10.1037/0033-2909.101.2.192
Walquist-Sørli, L., Caglar-Ryeng, Ø., Furnes, B., Nergård-Nilssen, T., Donolato, E., & Melby-Lervåg, M. (2025). Are speech sound difficulties risk factors for difficulties in language and reading skills? A systematic review and meta-analysis. Journal of Speech, Language, and Hearing Research, 68(1), 164–177. https://doi.org/10.1044/2024_JSLHR-24-00170
Weiner, F. F. (1981). Treatment of phonological disability using the method of meaningful minimal contrast: Two case studies. Journal of Speech and Hearing Disorders, 46(1), 97–103. https://doi.org/10.1044/jshd.4601.97
Williams, A. L. (2003a). Speech disorders resource guide for preschool children. Delmar Learning.
Williams, A. L. (2003b). Target selection and treatment outcomes. Perspectives of the ASHA Special Interest Groups, 10(1), 12–16. https://doi.org/10.1044/lle10.1.12
Williams, A. L., McLeod, S., & McCauley, R. J. (2010). Direct speech production intervention. In A. L. Williams, S. McLeod, & R. J. McCauley (Eds.), Interventions for speech sound disorders in children (pp. 27–39). Brookes.
Wolfe, V., Presley, C., & Mesaris, J. (2003). The importance of sound identification training in phonological intervention. American Journal of Speech-Language Pathology, 12(3), 282–288. https://doi.org/10.1044/1058-0360(2003/074)
World Health Organization. (2001). International classification of functioning, disability and health.
Wren, Y., Miller, L. L., Peters, T. J., Emond, A., & Roulstone, S. (2016). Prevalence and predictors of persistent speech sound disorder at eight years old: Findings from a population cohort study. Journal of Speech, Language, and Hearing Research, 59(4), 647–673. https://doi.org/10.1044/2015_JSLHR-S-14-0282
Wren, Y. E., Roulstone, S. E., & Miller, L. L. (2012). Distinguishing groups of children with persistent speech disorder: Findings from a prospective population study. Logopedics Phoniatrics Vocology, 37(1), 1–10. https://doi.org/10.3109/14015439.2011.625973
Acknowledgments
Content for ASHA’s Practice Portal is developed through a comprehensive process that includes multiple rounds of subject matter expert input and review. ASHA extends its gratitude to the following subject matter experts who were involved in the development of the Speech Sound Disorders: Articulation and Phonology page:
Primary Version
- Elise Baker, PhD
- John Bernthal, PhD, CCC-A/SLP
- Caroline Bowen, PhD
- Sharon Hart, PhD, CCC-SLP
- Barbara Hodson, PhD, CCC-SLP
- Sharynne McLeod, PhD
- Susan Rvachew, PhD, S-LP(C)
- Cheryl Sancibrian, MS, CCC-SLP
- Judith Trost-Cardamone, PhD, CCC-SLP
- Lynn Williams, PhD, CCC-SLP
Subsequent Versions
- Shanna Caprice Lee-Holloway, PhD, CCC-SLP (2025)
- Cynthia Core, PhD, CCC-SLP (2019)
- Kelly Farquharson, PhD, CCC-SLP (2025)
- Raul Prezas, PhD, CCC-SLP (2025)
- Elizabeth Roepke, PhD, CCC-SLP (2025)
- Holly Storkel, PhD, CCC-SLP (2019)
ASHA seeks input from subject matter experts representing differing perspectives and backgrounds. At times a subject matter expert may request to have their name removed from our acknowledgment. We continue to appreciate their work.
Citing Practice Portal Pages
The recommended citation for this Practice Portal page is:
American Speech-Language-Hearing Association. (n.d.). Speech sound disorders: Articulation and phonology [Practice portal]. https://www.asha.org/practice-portal/clinical-topics/articulation-and-phonology/
Content Disclaimer: The Practice Portal, ASHA policy documents, and guidelines contain information for use in all settings; however, members must consider all applicable local, state and federal requirements when applying the information in their specific work setting.











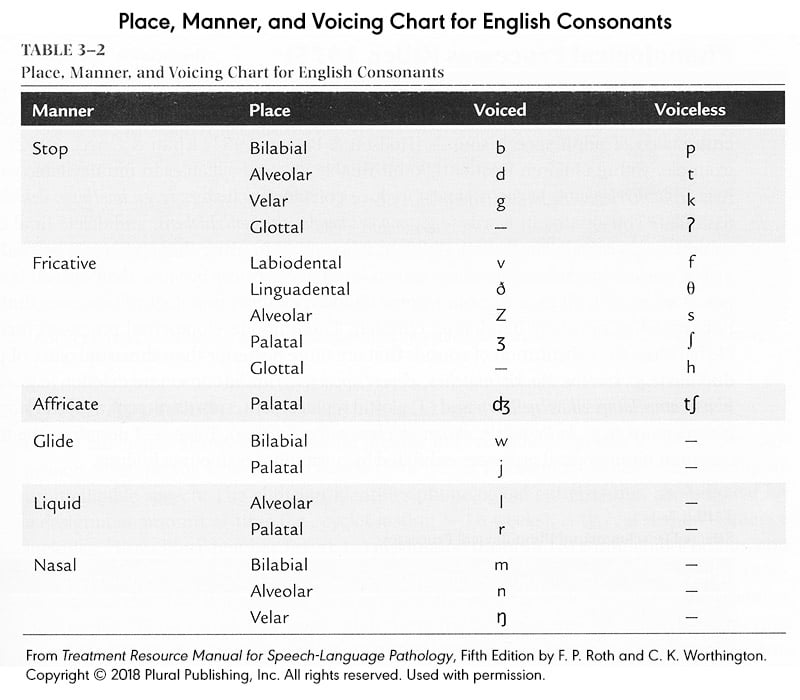{kind=link}